

1. Introduction: Two Paradigms of Central Nervous System Health
Multiple Sclerosis (MS) is traditionally defined as a chronic, idiopathic, immune-mediated inflammatory disease of the Central Nervous System (CNS). In the clinical environment, we often approach this condition through two distinct but increasingly intersecting paradigms. The first is the “Disease Management” approach, which focuses on modulating the immune response to prevent demyelination. The second is the “Structural Environment” approach, which prioritizes the biomechanical integrity of the spine—specifically the craniocervical junction—to ensure the nervous system can function without mechanical obstruction.
Learning Objective: Students will synthesize the traditional autoimmune model of MS with the biomechanical model of vertebral subluxation to understand how structural correction of the craniocervical junction (CCJ) influences neurovascular dynamics and clinical outcomes.
While the autoimmune cascade describes the inflammatory “fire” that damages the myelin sheath, we must first master the traditional model to appreciate why the “ventilation system”—the biomechanical structures that dictate how the CNS clears that inflammatory heat—is equally critical.
2. The Traditional Model: Immune-Mediated Pathophysiology
The prevailing medical understanding of MS centers on a dysfunction of the body’s adaptive immune system. In Relapsing-Remitting Multiple Sclerosis (RRMS), this manifest as acute episodes of neurological deficit followed by periods of partial or complete recovery.
The Autoimmune Cascade
Immune Dysregulation: The immune system loses self-tolerance, mistakenly identifying CNS antigens as foreign threats.
Targeting Myelin: Autoreactive B-cells and T-cells infiltrate the CNS, specifically attacking the myelin sheath, the lipid-rich insulation required for saltatory conduction.
Demyelination & Lesion Formation: This localized attack produces inflammatory plaques or lesions. In our case context, these are typically observed in supratentorial periventricular regions and the cervical spinal cord (e.g., at the C4–C5 level).
Signal Disruption: Demyelination causes “conduction block” or slowed signal transmission, resulting in the diverse neurological deficits seen in MS.
Clinical Presentation: Patients present with symptoms such as profound fatigue, disequilibrium, paresthesia, and gait instability.
Intervention Strategy: Modern management relies heavily on Disease-Modifying Therapies (DMTs). Agents like ofatumumab (Kesimpta), a B-cell depleting monoclonal antibody, target CD20-positive B cells to suppress the autoimmune activity responsible for new lesion formation. However, these pharmacological agents focus strictly on the immune response and are physically incapable of addressing functional biomechanical deficits.
3. The Biomechanical Model: Vertebral Subluxation and the CCJ
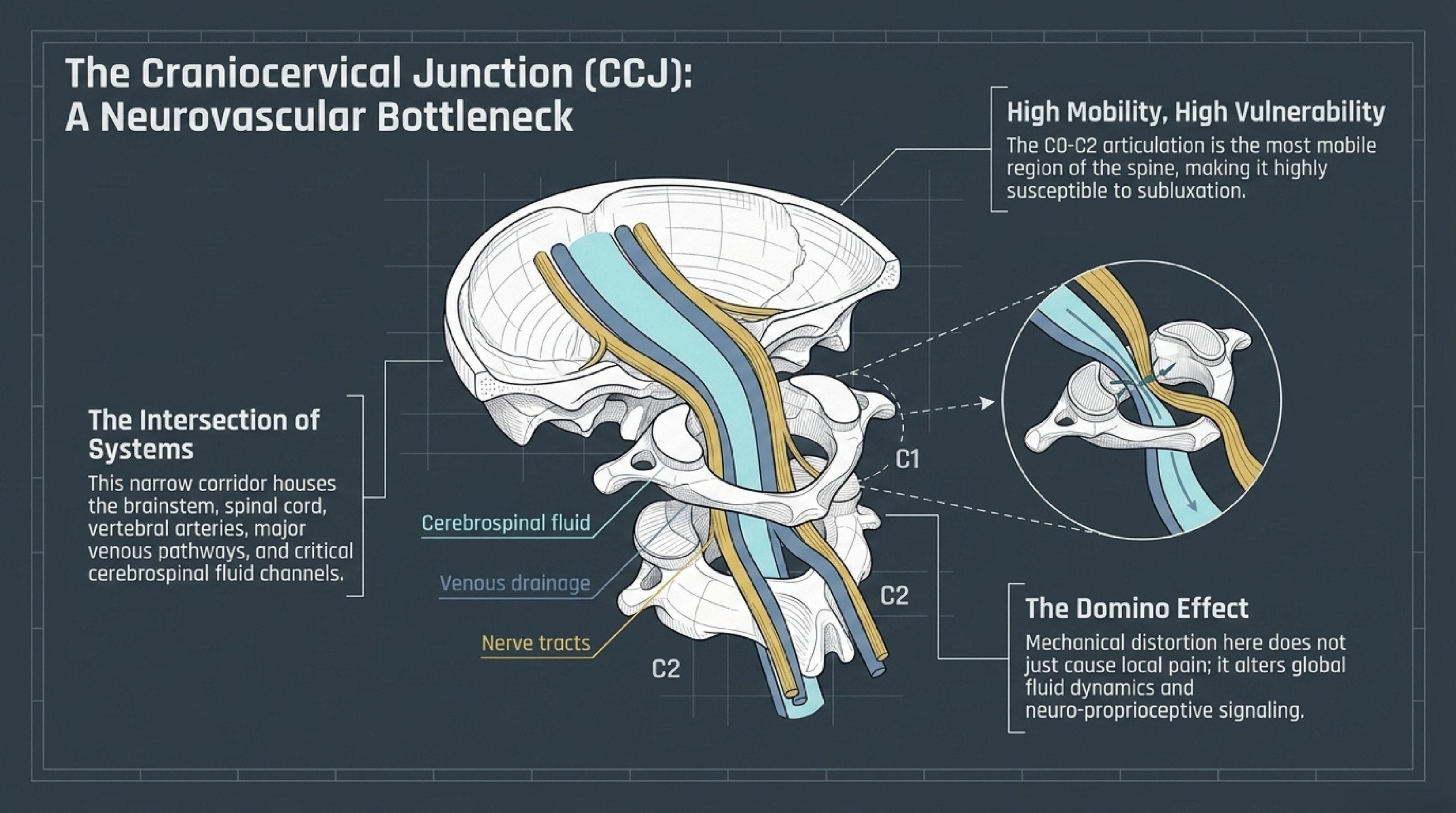
From a pathophysiological standpoint, we must view the Craniocervical Junction (CCJ)—comprising the C0–C2 complex (occiput, atlas, and axis)—as the primary neurovascular bottleneck of the central nervous system. A Vertebral Subluxation in this region is a structural shift that creates mechanical stress, obstructing nerve signaling and fluid dynamics. When the atlas (C1) loses its optimal alignment, it doesn’t just affect the bone; it alters the entire “plumbing” of the brain.
Neurophysiological Impact of CCJ Subluxation
Mechanism
Normal Function
Subluxated Dysfunction
CSF Hydrodynamics
Pulsates freely across the foramen magnum to drive perivascular movement and glymphatic clearance.
Mechanical tension creates resistance, leading to “sluggish” waste clearance and the accumulation of metabolic debris.
Venous Drainage
The Internal Jugular Veins (IJVs) efficiently drain deoxygenated blood from the brain.
Because the IJV passes in close proximity to the transverse processes of C1, subluxation causes functional stenosis and venous congestion.
Proprioceptive Signaling
Dense mechanoreceptors in the upper neck provide accurate afferent data for balance and coordination.
Aberrant signaling creates a vestibulocerebellar mismatch, manifesting as vertigo, dizziness, and gait instability.
This structural misalignment compromises intracranial compliance. A stagnant environment prevents the clearance of the very inflammatory mediators produced by the autoimmune cascade, potentially exacerbating the demyelination process.
4. Comparative Analysis: Managing the Disease vs. Supporting the Environment
The “so what?” for the clinician lies in the realization that biomechanical interference may actively hinder the resolution of an inflammatory phase. While medication addresses the “chemistry” of the attack, chiropractic care addresses the “architecture” of the recovery.
Focus Area
Immune-Mediated Paradigm
Biomechanical Paradigm
Primary Goal
Suppress autoimmune activity; prevent new lesions.
Reduce mechanical interference; restore neurovascular patency.
Intervention Type
Pharmacological (e.g., Kesimpta immunotherapy).
Structural (e.g., Atlas Orthogonal/Full-Spine).
Proposed Impact
Reduced B-cell mediated damage to myelin.
Improved CSF flow, venous drainage, and proprioceptive integration.
Clinical Focus
Managing the disease process (DMT).
Supporting the CNS environment and healing capacity.
Synthesis: A patient may be “stable” on medication yet still experience functional decline because the drug cannot restore cervical lordosis or clear venous congestion caused by a malpositioned atlas.
5. Integrated Clinical Insight: Evidence from the Field
The synergistic potential of these models is best demonstrated by a 30-year-old male RRMS patient. Crucially, during his first six months of Kesimpta-only therapy, his condition subjectively worsened, and MRI imaging showed disease progression, including the enlargement of a cervical lesion. It was only after the introduction of Atlas Orthogonal (AO) care to correct a confirmed C1 subluxation and reduced cervical lordosis that the clinical trajectory reversed.
3 Key Lessons from Integrated Care
Synergy in Resolution: Following AO intervention, the patient achieved a 72.7% reduction in overall symptom burden (QVAS/OATS) and a 75.8% reduction in fatigue (MFIS), reaching a “Very Much Improved” status that medication alone failed to achieve.
Structural Influence on Lesion Pathology: Most notably, follow-up MRI demonstrated a reduction in T2-weighted signal intensity at the C4–C5 lesion and reported no new lesions. This suggests that improving fluid dynamics (clearing the “stagnant” environment) may support the resolution of active inflammatory phases.
Neurovascular Patency: The sensation of “release” reported by the patient during atlas correction aligns with the restoration of venous drainage and the alleviation of mechanical pressure on the brainstem and spinal cord.
6. Summary: The Future of Integrative Neurological Health
We must teach our students that chiropractic care is a complementary discipline, not a cure for MS. It does not target the idiopathic disease process itself; rather, it optimizes the structural environment in which the nervous system must operate. By correcting the C0–C2 complex and restoring intracranial compliance, we reduce the mechanical stress that hinders the body’s innate ability to adapt to the physiological challenges of Multiple Sclerosis.
Student Quick-Reference While immune-mediated management focuses on pharmacological suppression of the autoimmune attack on myelin, the biomechanical paradigm seeks to remove structural obstructions at the craniocervical junction to optimize fluid dynamics and neurological signaling. This integrative approach ensures that the body’s ventilation and drainage systems are functional enough to support the resolution of the inflammatory heat generated by the disease.
CLICK HERE for related research
